MALARIA CONTROL
AND MANAGEMENT
Malaria prevailed for centuries ranging from severe epidemic and at a tipping point in 1930s to near elimination in 1960s and resurgence after 1970’s. Many national and international non-governmental organizations (NGOs), research institutions and donors are also involved in malaria control. Financing agencies such as WHO and Global Fund together with health-care staff in remote areas, excellent policies and intelligent investments in health care, with the unstinted support of technical have been able to achieve a malaria free status.
ESTABLISHMENT OF ANTI-MALARIA CAMPAIGN (AMC)
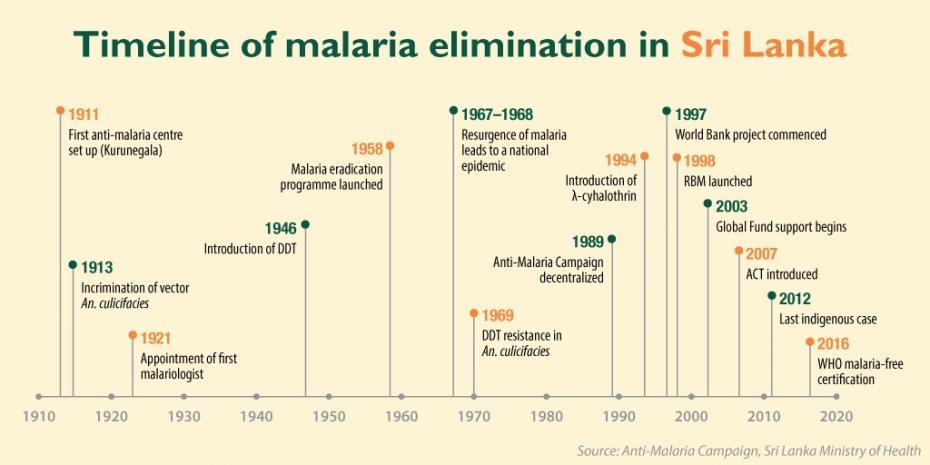
The first Anti-malaria campaign was set up in Kurunegala town to eradicate Malaria prevailing in the country. The Anti-Malaria Campaign (AMC), Sri Lanka’s National Malaria Control Programme was established as a field office in 1911. They conduct a specialized programme which formulates policies, monitor, provide technical guidance to regional malaria offices, co-ordinate research and oversees surveillance. There are 20 regional malaria offices throughout the country.
ROLE OF WHO
The WHO Global Malaria Programme (GMP) is responsible for charting the course for malaria control and elimination by setting, communicating and promoting the adoption of evidence-based norms, standards, policies, technical strategies, and guidelines, keeping independent score of global progress; developing approaches for capacity building, systems strengthening, and surveillance and identifying threats to malaria control and elimination as well as new areas for action.
PREVENTION OF RE-INTRODUCTION AND CONTROL OF MALARIA
The biggest threat for the elimination efforts is the risk of resurgence due to imported malaria cases and also Sri Lanka being a tropical country is a favourable breeding ground for the vectors as it has many high vulnerability and high receptivity areas. The following strategies are used to prevent re-introduction and control outbreak
- Parasitological surveillances
- Entomological surveillance (sentinel site surveys ,random spot surveys and case based surveys)
- Vector control
- Pharmacological vigilance for anti-malaria medicines
- Public awareness
ERADICATION OF MALARIA
Malaria control activities began during the British rule itself. In the beginning Anti larval measures (application of copper aceto arsenite Paris green) and environmental measures were effective in urban areas but in rural areas due to breeding grounds the disease spread swiftly. During the massive outbreak in 1930s Quinine was the main drug used for treatment
INTRODUCTION OF DDT
In 1946 it was a major achievement after Dichlorodiphenyltrichloroethane (DDT) was introduced in the country after which there was a major decline in malaria morbidity and mortality and the malaria situation was reasonably well controlled. The parasite incidence reached a remarkably low-point which included only few indigenous cases (rest were imported). Due to the favorable indicators, spraying was halted throughout the country except spraying was carried over on a few affected areas. There was a resurgence of malaria after being halted and later DDT was resistance to malaria
INTRODUCTION OF MALATHION
Later indoor residual spraying (IRS) was used for elimination and treatment of patients with chloroquine and primaquine. As there was an increase in DDT resistance there were more severe forms of Malaria and Malathion was introduced as an alternative in 1975. The control activities were highly effective with IRS and Malathion which were supplemented with other vector control methods such as larviciding, case detection and treatment, expansion of laboratories services, entomological studies and awareness programmes to the public. Chloroquine-resistant P.falciparum first detected and then malaria was decentralized. The regional malaria clinics improved diagnosis and treatment. Then in 1984 Widespread Malathion resistance in An. culicifacies detected
INTRODUCTION OF ARTEMISININ-BASED COMBINATION THERAPY (ACT)
At the beginning of the century with intensified control measures and well-trained health care workers, surveillance and treatment were made more efficient. Insecticide-treated mosquito nets were introduced and there was a gradual decline in the 2000s. Plasmodium falciparum and Plasmodium vivax were going down. In 2008 artemisinin-based combination therapy (ACT) was introduced which was a huge success after which there were no deaths reported. Malaria elimination Projects were established in order to eliminate Malaria and finally eradicated in the year 2012.